https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/implantable-acoustic-devices-iads/
Implantable acoustic devices (IADs)
This webpage describes the type of IADs used at Great Ormond Street Hospital (GOSH), what is involved in fitting them and what to expect during treatment.
How do IADs work?
Like conventional hearing aids, IADs stimulate the hearing organ in response to sounds. However, instead of transmitting sound through the ear canal, IADs transmit sounds as vibrations through the skull and middle ear bones to the inner ear.
IADs may also be called BCIs (bone conduction implants) or BAHAs (bone anchored hearing aids).
Who are IADs suitable for?
IADs are usually suggested for people who:
- Can’t use conventional hearing aids because their ear canal or the outside parts of the ear haven’t developed.
- Have a certain type and level of hearing loss.
What types of IADs are available?
There are four types of IADs available at GOSH:
Percutaneous BCI:
An abutment (a small metal connector) is attached to the skull and comes through the skin. The abutment can be connected to a sound processor which sits on the outside of the head. The sound processor looks like a small box and vibrates to send the sound signal through the abutment and skull to the inner ear.
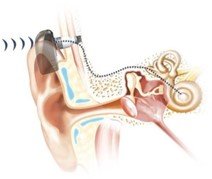
Percutaneous BCI
Magnet BCI/ Passive transcutaneous BCI:
A magnet about the size and shape of a two pence coin is implanted under the skin. A sound processor sits on the outside of the head. They are held together by magnetic attraction. The sound processor sends vibrations through the skin to the internal magnet and then to the skull and the inner ear.
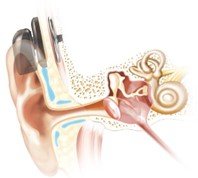
A magnetic BCI
Active transcutaneous BCI:
This also sits completely under the skin. However, unlike the abutment and magnet BCI, the implant (the internal part) produces the vibrations rather than the sound processor (the external part). An external sound processor is held in place using a weak magnet and tells the internal implant what sounds to produce.
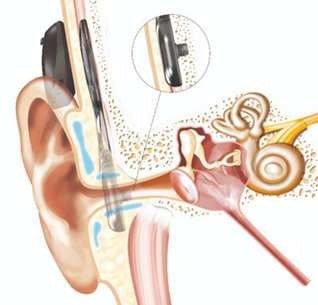
Active BCI
Middle ear implant (MEI):
This works similarly to an active transcutaneous BCI, however it sends sounds directly to the inner ear via the bones in the middle ear, rather than the skull.
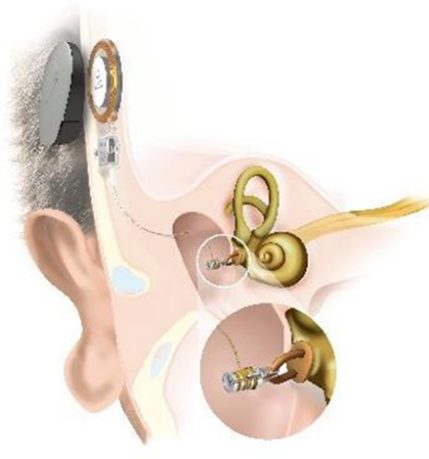
Middle ear implant
What are the advantages or disadvantages of each type of IAD?
Your child’s Audiologist and Ear Nose and Throat (ENT) surgeon will discuss suitable options with you. Your child may not be suitable for all types of implant.
Please note: the following lists are not exhaustive but provide an overview.
Device examples: BAHA Connect or Ponto
Pros:
- Better hearing outcomes.
- Can still have magnetic resonance imaging (MRI) scans.
Cons:
- Risk of complications at the implant site, such as skin irritation and infection.
- You can’t swim whilst using the processor.
Device examples: BAHA Attract
Pros:
- As the magnet is under the skin there’s a lower risk of implant site complications.
Cons:
- Precautions must be taken when undergoing MRI scans.
- Less favourable hearing outcomes.
- You can’t swim whilst using the processor.
Device examples: Osia or Bonebridge
Pros:
- The implant is under the skin so there is a lower risk of implant site complications.
- Better hearing outcomes.
- Weaker magnet required so there is a lower risk of skin irritation.
- You can swim with the processor if appropriate casing is used.
Cons:
- Precautions must be taken when undergoing MRI scans.
- If the implant needs to be replaced, this will involve a further surgery.
Device examples: Soundbridge
Pros:
- The implant is under the skin so there’s lower risk of implant site complications.
- Better hearing outcomes.
- You can hear what direction sounds come from.
- Weaker magnet required so there is a lower risk of skin irritation.
- You can swim with the processor if appropriate casing is used.
Cons:
- Precautions must be taken when undergoing MRI scans.
- Greater complexity of surgery.
- If the implant needs to be replaced, this will involve a further surgery.
How will you decide if an IAD is right for my child?
We will look at your child’s hearing tests and the condition of their hearing. A CT scan may also be recommended.
We will also often recommend trialing a bone conduction hearing aid secured with a head band for a few weeks. This can give us an indication of whether your child will benefit from an IAD.
Depending on your child’s age, the soft band may also be a temporary measure until they are old enough for the operation.
- If the trial is successful, the Audiologist will make an appointment for you to see the ENT surgeon to discuss the options.
- If the trial is not successful, an IAD will not be the best option for your child so other treatments may be discussed.
About the IAD surgery
Your child’s ENT surgeon will discuss the surgery with you both in a clinic appointment and on the day of surgery. They will answer any questions and ask you to give permission for the operation by signing a consent form.
The operation will be carried out while your child is under general anaesthetic (they will be asleep). An anaesthetist will talk you through this on the day of surgery.
What will the operation involve?
- We may need to shave a small amount of hair.
- The surgeon will then make a small 2-3cm incision (cut) behind the ear and fix the implant to the skull.
- The skin is stitched around the abutment, which comes through the skin.
- A ‘healing cap’ or protective cover will be put over the abutment to protect it while it heals.

Healing cap
- We may need to shave a small amount of hair.
- The surgeon will then make a C-shaped incision (cut) where the magnet will be placed and fix the magnet to the skull.
- They will then stitch up the incision and cover it with a bandage.
- We may need to shave a small amount of hair.
- The surgeon will make an L-shaped incision around the lower part of where the implant will go.
- The implant will then be inserted and secured to the skull.
- They will then stitch up the incision and cover it with a bandage.
- We may need to shave a small amount of hair.
- The surgeon will make a C-shaped incision behind the ear.
- The surgeon will remove some of the mastoid bone behind the ear, near the nerve that moves the face.
- The surgeon will find the hearing bones in the middle ear.
- They will secure the device to the skull and then attach it to the hearing bones in the middle ear.
- The incision is then stitched up and covered with a head bandage.
Rarely, some operations are conducted over two stages.
What are the risks of IAD surgery?
All surgery and anaesthesia carries a degree of risk but we will do everything we can to minimise it.
The risk of the anaesthetic will depend on your child’s medical condition(s). Risks cannot be removed completely but modern equipment, training and medicines have continued to make anaesthesia safer. An anaesthetist will be with your child throughout their anaesthetic to monitor their progress and to help them to wake up as comfortably as possible.
There is a risk of bleeding and possible infection with any operation. Blood loss during surgery is usually minimal and we may give your child antibiotics to reduce the risk of infection. If implants become infected, they may need to be removed to allow the body to heal, before they are reinserted at a later date.
The implants may occasionally become loose from the skull bone - this is often connected to an infection in the area.
Middle ear implants are more complex operations and therefore have greater risks. Specifically, there are very small chances of causing a hearing loss in the inner ear and of injuring the nerve that moves the face.
There is also a risk that your child may not find adequate hearing benefit from the auditory implant.
Going home after the operation
If your child is recovering well from the surgery and anaesthetic, they will be able to go home later on the day of surgery or the following day.
We may give your child a course of antibiotics to reduce the risk of infection. Please complete the course of antibiotics even if your child is feeling better.
For some children the surgical site will still be a bit swollen and uncomfortable when they get home. Carry on giving your child paracetamol and/or ibuprofen pain relief according to the instructions on the bottle or packet.
Looking after the operation site
Keep the wound clean and dry for the first 10 days after the operation. After this, take care when hair washing or brushing.
The sticky paper stitches will fall off in a few days - the other stitches are dissolvable so will not need to be removed.
Your child should not go swimming or take part in sports or PE lessons until they have seen the ENT surgeon at their follow-up appointment.
If your child had a percutaneous BCI inserted, there will be a dressing under the healing cap. Do not remove this until the ENT appointment one week after the operation - at this appointment the dressing may be replaced.
What should I do if I think there is an infection?
Signs of infection include:
- Your child is in a lot of pain and pain relief does not seem to help.
- Your child has a temperature of 38°C or higher.
- The operation site is red or inflamed and feels hotter than the surrounding skin.
- There is an unpleasant smell or ooze from the operation site.
If you see any signs of infection, take your child to the nearest Accident and Emergency (A&E) department immediately, or to a GP if they are able to be seen urgently (on the same day).
During office hours, you can also ring the ENT secretaries on 020 7813 8220 to arrange a review or to get advice from a member of the ENT team.
Follow up appointments
We will make a follow up appointment with the ENT surgeon a few weeks after the operation.
An audiology appointment will be booked for approximately one to three months after the operation, depending on which surgery your child has.
Fitting the hearing processor
Once the wound has healed, the hearing processor will be fitted and reprogrammed. This may be the same processor that was fitted on the soft band in the trial.
Whilst you’re waiting for this fitting, your ENT surgeon can advise whether your child should continue using the soft band. Do not attempt to put the soft band processor onto the implant as this may damage the integration.
The fitting appointment will involve either reprogramming your child’s existing device to work well with their new implant, or providing a new processor. When using a magnet fixture, the audiologist may need to trial different strengths to find out which one is most suitable for your child. The magnet needs to be strong enough to stay on but not too tight that it will cause complications.
Once your child has been using the hearing device for a few weeks, the Audiologist will continue to assess your child's hearing with the BCI and arrange appropriate follow ups.