https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/feeding-your-child-after-oesophageal-atresia-andor-tracheo-oesophageal-fistula-repair/
Oesophageal atresia (OA) and tracheo-oesophageal fistula (TOF): Feeding after repair surgery
If you would like this information in another language or format, please contact the Patient Advice and Liaison Service (PALS).
This webpage explains how to safely wean and feed your child after an OA or TOF repair operation. This information is based on specialist experience of looking after children with OA and TOF and promotes safe feeding practices.
Note: Whilst we mention specific brands, this is not an endorsement- other options including supermarket own-brands may be just as suitable.
What is OA and TOF?
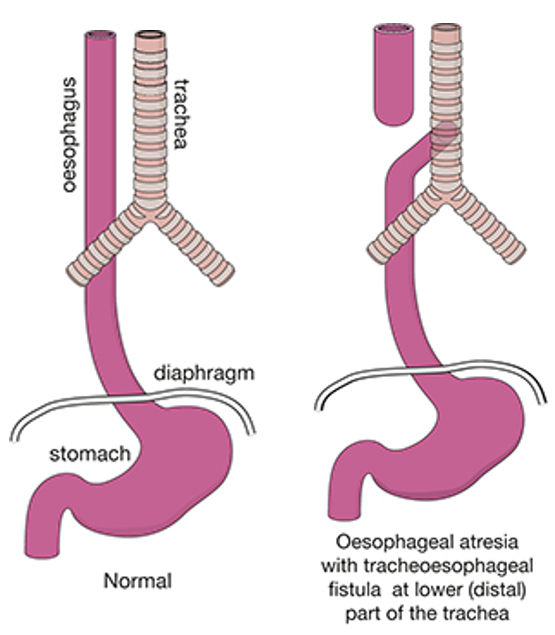
Oesophageal atresia (OA) is a rare condition where a short section at the top of the oesophagus (gullet or food pipe) has not formed properly so is not connected to the stomach. This means food cannot pass from the throat to the stomach.
Tracheo-oesophageal fistula (TOF) is another rare condition, which tends to occur alongside oesophageal atresia. This is where part of the oesophagus is joined to the trachea (windpipe).
Both conditions are usually diagnosed soon after birth or occasionally before birth by a scan. Both conditions require repair with an operation.
Why might my child have difficulty with food?
Some children with OA/TOF find weaning and feeding straightforward, whereas for others difficulties can occur. Children with OA/TOF might have difficulties with feeding because of:
- Oesophageal incoordination/dysmotility: Normally, the oesophagus squeezes food down towards the stomach using an action called ‘peristalsis’. In OA/TOF this does not work effectively which means that food may move up, as well as down, the oesophagus, take longer to go down or get stuck.
- Oro-pharyngeal dysphagia: This means swallowing difficulties related to the mouth and throat. Children with OA/TOF may experience coughing with eating or drinking because of coordination difficulties in the throat that mean food or drink can more easily ‘go down the wrong way’.
- Gastro-oesophageal reflux: Due to the coordination problems, reflux is also common in children following OA/TOF repair. Reflux is where acid from the stomach can travel back up the oesophagus causing discomfort and sometimes vomiting or choking. At GOSH we recommend that all children with OA/TOF are treated with anti-reflux medication.
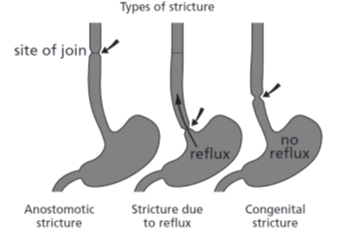
- Stricture: This is a narrowing of the oesophagus. This can happen due to scar tissue from the operation or due to gastro-oesophageal reflux where the contents of the stomach flows back up the oesophagus rather than out of the stomach. Very rarely, children are born with a stricture. If the oesophagus is narrowed, it may be difficult for food to pass through this section so may get stuck.
- Delayed repair: Children may have a delayed repair, often because the gap between the two ends of the oesophagus is too long to repair in one operation. They will usually be fed through a tube directly into their stomach. This means that they might be slower to start feeding by mouth because they are not used to it or sometimes because they associate their mouth with uncomfortable procedures.
Starting milk feeds
A few days after the operation, when the doctors are happy that your child’s bowel is ready, they may suggest starting nasogastric (NG) feeding. An NG tube is a flexible tube that goes up nostril and down the oesophagus into the stomach. You may also hear it referred to as a trans anastomotic tube or TAT. An NG can be used to help remove (vent) any air from the stomach, which could be making your child uncomfortable, and to give your child feeds directly into their stomach.
Initially, your child can have expressed breast milk or formula given slowly via the NG tube into their stomach. They can continue to have NG feeds until the team thinks your child is ready to start having milk by mouth.
Your child will continue with milk feeds until they are ready to start weaning (introducing food). If you have any worries about your feeding or swallowing skills, please contact your clinical team- they will arrange an assessment with a Speech and Language Therapist and/or a Dietitian if needed.
Weaning onto smooth purees
Most babies begin to develop head control and increased body strength by the age of six months. At this stage, they can start trying smooth pureed food. We advise to not start weaning until you have discussed it with your child’s surgical consultant. You should have an appointment with them at around this time.
Puree textures
The International Dysphagia Diet Standardisation Initiative (IDDSI) is a scale designed to show the texture of foods and liquids. Children with OA/TOF should start weaning at level three (as shown on the diagram).
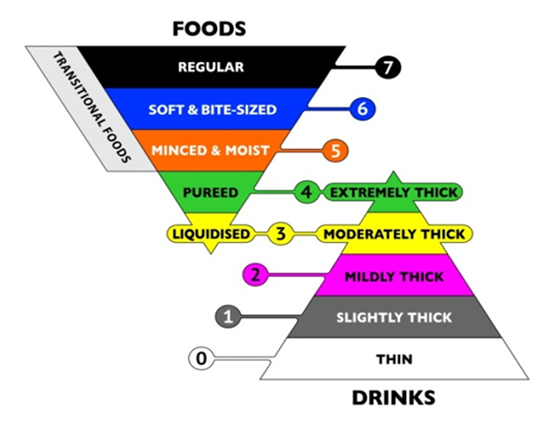
International Dysphagia Diet Standardisation Initiative (IDDSI) scale
How should I start introducing purees?
To start with, thin down the puree using your child’s usual milk feed so that it is only slightly thicker than your child’s usual milk. The first foods are more to introduce tastes rather than to provide nourishment, so aim for just a few small spoonfuls. Stick to just one or two tastes for the first few days, to help you see how your child is coping and which purees your baby does well with.
Over the next two weeks gradually increase the thickness of the puree by adding less liquid. You are aiming for IDDSI level 3 (liquidised)- this is pureed food that will drip through the prongs of a fork. When you know they are coping with the slightly thickened purees, you can start to introduce new tastes. Your child may pull faces or be unimpressed when they first try a new taste- this is normal. Try the taste on a few more occasions before you rule it out.
Suitable first weaning (IDDSI level 3) foods to try include:
- Baby rice or cereal mixed with your child’s usual milk.
- Well-cooked then liquidised vegetables and fruit, such as swede, broccoli, cauliflower, apple or pear.
- Liquidised fresh fruit such as banana, strawberries or blueberries.
- Fromage frais or yoghurt without ‘bits’.
- Stage 1 baby foods (these are those labelled as suitable for babies aged between four and six months).
Children with OA/TOF often make different sounds when they are eating- this can be due to tracheomalacia (a weak or soft windpipe). If your child coughs when feeding, or sounds wheezy during and after feeds, call your child’s medical team. They may advise a review with a Speech and Language Therapist.
Tips for weaning
- Choose a time when your child is wide awake but not over-hungry.
- Let your child play with their food, touch it and spread it around. Let them put their hands in their mouths. Give them their own spoon that has been dipped in food so they can start to feed themselves. Wait until they have finished eating and playing before you start to clean up and wipe them down.
- Families have told us it is often easier to batch cook large amounts of a wide range of pureed foods which can then be frozen in portion sizes.
- Children may find their meals more appealing if the different foods are pureed separately and put on the plate or bowl separately too. This means the foods stay a similar colour and flavour as they would be in solid form. Mixing food together before pureeing can result in a grey stodge!
A blender will help make foods very smooth.
Introducing drinks
As your child moves from thin purees to slightly thicker ones, give them some water to drink alongside. A cup without a lid is best as this will help your child to develop the skill of sipping. You can use sippy cups, but we advise that you remove the top. No spill cups are not suitable as they need to be sucked so don’t encourage your child to learn to sip. When out and about a 360 cup is a good alternative to a non-spill sippy cup. There are lots of brands available online and from department stores. Learning to sip water is important as the water acts a lubricant for more solid foods as your child’s weaning progresses.
Moving on to thicker purees
Once your child is managing thin purees and sips of water, you can reduce the amount of milk you add so the purees become a bit thicker. This level of puree will hold its shape on a spoon but will fall off in one dollop when the spoon is tilted.
Suitable thick purees (IDDSI level 4) foods to try include:
- Similar foods to level 3 but with less milk feed added.
- Pureed meat and fish or pulses such as lentils and beans.
Introducing food with texture
At around the one year of age, your child may be ready to try more textured stage 2 baby foods. The clinical team will review your child and discuss this with you before giving you the go ahead.
These foods can contain ‘bits’ but they should be very small- no bigger than 2mm by 2mm to start off with. Foods should also be soft enough to mash easily with a fork.
Suitable (minced and moist) IDDSI level 5 foods to try include:
- Pureed fruit such as strawberries or raspberries leaving in a few small seeds.
- Add some couscous, quinoa or crushed Rice Crispies™ to a level 4 food to add a bit of texture.
- Pureed meat and fish or pulses such as lentils and beans or egg.
- Stage 2 baby foods- make sure they are described as textured rather than lumpy. If the ‘bits’ in it are too large, you may have to mash them down a bit before giving to your child.
Typically, babies move on to increasingly textured foods at eight to nine months, however children with OA/TOF are at an increased risk of choking because of stricture/dysmotility. Therefore, we recommend that you progress slowly through the IDDSI stages as outlined in this guide. Only move onto the next stage once you are confident that that your child can handle the texture without any issues.
Moving on to solid foods
Please consult with your surgical team/CNS team before moving on to solid foods.
Introducing bite and dissolve foods
Your child will only learn to chew when they move on to firmer food textures. Bite and dissolve foods ‘melt’ in the mouth so your child can swallow them easily, but they still learn how to bite and chew.
We advise trying ‘bite and dissolve’ finger foods at around eight months of age. As well as eating skills, these will help your child develop hand-eye coordination by picking up foods and put them in their mouth.
There are lots of different types of bite and dissolve foods available. Try them yourself to judge how easy they dissolve before you give to your child. Many of these foods are available in the baby food aisle in a supermarket. Packets labelled “from six months” will melt most easily. You can also try foods such as smoothie ice lollies, or a ‘bite and dissolve’ crisp dipped in hummus.
Bite and dissolve foods are usually snack foods, so should not form a large part of your child’s diet.
Introducing more texture
When the clinical team is happy for you to introduce more textured foods, we suggest taking this in stages:
- Smooth thick purees- such as mashed potato or Weetabix® with less milk.
- Well-mashed foods- such as mashed banana or avocado.
- Small soft lumps in food- for example mashed potato with small pieces of soft cream cheese.
Tips
- Add sauces and gravy to foods to provide extra moisture to help swallowing.
- Adding water to food before pureeing it will dilute its nutritional benefit- try using milk, fruit juice, sauces, soup or gravy instead.
A balanced weaning diet
Try to aim for a balanced diet with plenty of variety:
- Starchy carbohydrates such as rice, cereals, porridge.
- Fruit and vegetables.
- Dairy products including milk, yoghurt, cheese.
- Fats such as oils and spreads.
- Proteins such as meats, poultry, Quorn™, fish, eggs, beans, pulses.
To make sure your child’s diet is nutritious, try to include protein sources even though they may be trickier to puree to the correct consistency. Fibrous protein foods, such as meat, are best pureed when they are well cooked and tender.
Problem foods
Some foods are particularly problematic for children following OA/TOF repair as they tend to get stuck and cause blockages. Avoid these foods:
- Doughy foods such as bread, doughnuts, pastries and thick crust pizza.
- Raw apples and raw vegetables.
- Citrus fruits, due to the pith (white stringy substance).
- Hot dogs, frankfurters and sausages.
- Lumps of meat, poultry or Quorn™ that need a lot of chewing or are stringy- we advise you continue to puree meat even if your child is eating non-pureed vegetables or pasta. You can introduce non-pureed meat, but it should be minced or chopped very finely and mixed with a sauce.
The following foods may be difficult for other reasons:
- Slippery food that might be swallowed too quickly- such as peaches or grapes.
- Rusks- although they are soft when chewed they can form a difficult-to-swallow lump.
- Fibrous or stringy foods such as some cooked vegetables.
If you have any worries about your child’s feeding or swallowing or if their feeding with textured food changes or gets more difficult, this could be an indication of a stricture or another problem. Please contact your clinical team immediately- they will arrange assessment.
Dealing with reluctance
Children who struggle to eat (or have rarely eaten by mouth) can show reluctance to try new foods. This is particularly problematic with children who have had an OA/TOF repair as one bad experience with food can put them off for a long time.
The key is to carry on trying but to ask for help. There are lots of people at GOSH who can help- dietitians, speech and language therapists and we also have a specialised feeding disorders team.
Good days and bad days
Every child- whether they have OA/TOF or not- will have good days when they enjoy food and days when they seem to go backwards towards comforting foods that they know well. Children with OA/TOF may struggle if they are unwell, for instance with a cold or sniffles, or are teething.
You may worry that a setback means something more serious, such as a stricture. If you are concerned, contact your clinical team for advice.
Otherwise, it is fine to go back a step when your child is unwell and then reintroduce the next stage when they feel better.
We recommend keeping a supply of ‘easy to eat’ foods such as soups and milkshakes for these times.
What should I do if my child is coughing or choking?
If your child is coughing or food seems to get ‘stuck’ while eating and drinking, you should contact your clinical team for further assessment.
In an emergency, use the basic life support skills we have taught you while someone dials 999 for an ambulance.
Information and support
TOFS is a national charity and support group for anyone affected by OA/TOF.
You can call them on 0115 961 3092 or visit their website: TOFS website
Contact us
If you have any questions or concerns, please contact the Specialist Neonatal and Paediatric Surgery (SNAPS) CNS team.
Phone: 02074059200 ext 5092/5093 Monday to Friday, 9am to 5pm.
Or email: surgical.outreachteam@gosh.nhs.uk