https://www.gosh.nhs.uk/conditions-and-treatments/clinical-outcomes/neurodisability-clinical-outcomes/
Neurodisability clinical outcomes
If you would like this information in another language or format, please contact the Patient Advice and Liaison Service (PALS).
Clinical outcomes are measurable changes in health, function or quality of life that result from our care. Constant review of our clinical outcomes establishes standards against which to continuously improve all aspects of our practice.
About the Neurodisability Service
The Wolfson Neurodisability Service offers expertise in comprehensive assessment, diagnosis and advice on management of children with complex neurodevelopmental disorders.
The service is comprised of a number of specialist multidisciplinary teams, which can include consultants in paediatric neurodisability, paediatric neurologists, clinical nurse specialists, clinical psychologists, occupational therapists, physiotherapists, speech and language therapists, assistive technologists and administrative staff. We treat a wide range of conditions.
Osteogenesis imperfecta
Osteogenesis Imperfecta (OI) also known as ‘brittle bone disease’ is a rare genetic condition that is present from birth, where type 1 collagen (an important protein responsible for maintaining the structure of bone and other tissues, such as tendons, ligaments, skin and blood vessels) is deficient or of low quality. As a result, the minerals in the bone are not supported enough, which makes the bones weak and easy to break or crack, known as a fracture. There are different forms of the condition, from mild through to severe. People with mild forms may be minimally affected, while people with severe OI may experience many fractures throughout their lifetime, have misshapen bones, and require a wheelchair for mobility. The aims of multidisciplinary care and treatment include reduction in rate of fractures and complications, and optimisation of function and participation.
The OI Service at GOSH is one of four designated centres in England comprising the OI Highly Specialised Service for children and young people with Severe, Complex and Atypical OI. This service enables children and families to access high quality multi-specialty (neurosciences, endocrine, orthopaedic, radiology, clinical genetics, dentistry, occupational therapy, physiotherapy, nursing, psychology, social work), and multidisciplinary care nationally.
The clinical outcomes data published below are for this more significantly affected cohort of children, which comprise about one third of the total number of children and young people under the OI service at GOSH. All children within the OI service receive the same model of multidisciplinary care but may be seen less frequently if mildly affected.
Clinical outcome measures
Specific outcome measures were established nationally to measure the effectiveness of the Highly Specialised OI service, including:
1) Rate of Fracture
In OI, fractures can occur in any bone in the body, causing pain and in some cases residual bone deformity. Fractures can impact on day-to-day activities, school attendance and participation, movement and mobility until healing occurs.
2) Rate of progressive scoliosis
A proportion of children with OI develop curvature of the spine, known as scoliosis, which may change in shape with time and growth.
3) Rate of basilar invagination
This is a rare complication of OI that affects the alignment of the top of spine and base of the skull, which can lead to crowding of structures at the back of the brain and neurological symptoms.
With specialist multidisciplinary care, our aims are to reduce fracture risk, help rebuild compression fractures in the spine, and reduce rates of progressive scoliosis and basilar invagination over time through a combination of bone strengthening medicines, orthopaedic surgical interventions if needed, and the expertise and co-ordination of medical, therapy and nursing care.
1. Rate of fracture
| Measure |
GOSH 2022/23 |
GOSH 2023/24 |
GOSH 2024/25 |
National average 2022/23 to 2024/25 |
|---|---|---|---|---|
|
Percentage of patients in the service with confirmed non-vertebral fractures |
35% | 32% | 32% | 33% |
|
Percentage of patients in the service with vertebral fractures |
71% | 66% | 65% | 64% |
2. Rate of progressive scoliosis
| Measure |
GOSH 2022/23 |
GOSH 2023/24 |
GOSH 2024/25 |
National average 2022/23 to 2024/25 |
|---|---|---|---|---|
|
Percentage of patients with moderate scoliosis (Cobb angle 30-45°) |
4% | 5% | 5% | 5% |
| Percentage of patients with severe scoliosis (Cobb angle >45°) | 10% | 11% | 12% | 8% |
3. Rate of basilar invagination
| Measure |
GOSH 2022/23 |
GOSH 2023/24 |
GOSH 2024/25 |
National average 2022/23 to 2024/25 |
|---|---|---|---|---|
|
Percentage of patients in the service confirmed to have basilar invagination |
4% | 3% | 5% | 4% |
|
Percentage of patients not screened for basilar invagination |
0% | 0% | 0% | 9% |
4. Patient-reported outcome measure
Here, we provide our outcomes from the perspective of parents, carers (for patients aged under 12) and the young people themselves (aged 12 and over). This patient-reported outcome measure (PROM) gives us information about how our service assists with health-related knowledge and empowerment, and the effects of our care on daily living. Below is a selection of results for 2024/25.
Parents/carers (N=30):
- In the last 12 months at school, has input from the OI team helped your child in any of the following areas?
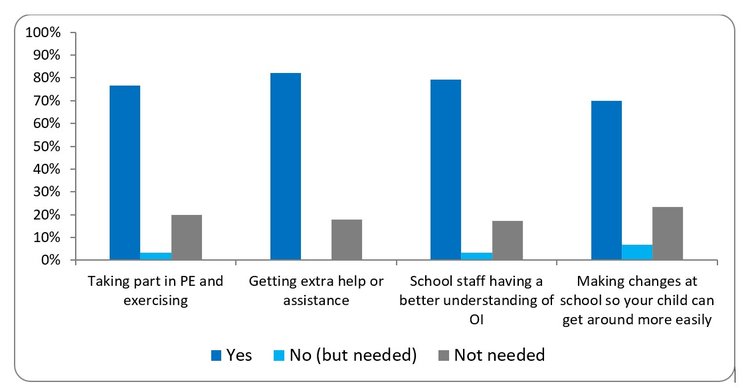
This bar chart is showing parent or carer responses about school support needs for children with OI. Around 70-80% said “yes” for support with PE and exercise, extra help, school staff having an understanding of OI, and making school changes for accessibility. A small percentage reported “no (but needed)”, and around 15 to 20% said support was “not needed”.
Having OI often leads to challenges for children, young people and families with regards to safe and inclusive participation in school life. Throughout the year the OI therapy team (Physiotherapists and Occupational Therapists) work collaboratively with education providers to assess the environment, support risk assessments and problem solve to ensure children and young people can access all areas of the curriculum. The results in the chart above indicate parents feel the input provided to schools has helped their child in the educational environment and the therapy team continue to evaluate this service via survey questionnaires sent to education providers.
2. At your most recent visit to hospital or to clinic, did you have a discussion with a member of the OI team about:
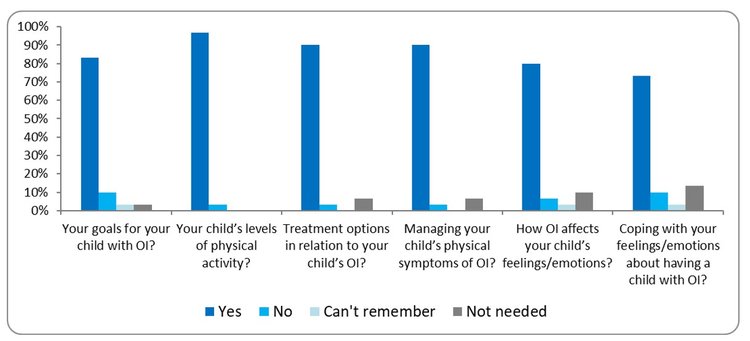
This bar chart is showing parent or carer responses about their most recent visit at the hospital or clinic and whether they were able to discuss with the OI team about their child with OI, covering goals, physical activity levels, treatment options, managing symptoms, feelings and emotions and coping with feelings and emotions. Around 80-95% said “yes” to being able to discuss these topics with the OI team. A small percentage reported “can't remember” and “not needed”.
The multidisciplinary team (MDT) clinic approach facilitates conversations around all aspects of the child or young person’s life, including physical health and emotional wellbeing. Support is further available from an OI Clinical Psychologist who can offer a space to talk about the condition and the impact it may have on everyday life, such as school, friendships and family relationships. During the year, groups are run to promote opportunities for parents and young people to meet and share their experiences, including baby/toddler groups and pain management groups.
3. Parent and carer communication and empowerment

This bar chart is showing parent and carer responses on communication and empowerment on whether they were able to have important questions answered by the OI team, views about their child’s care and treatment being listened to, involvement in decision-making about their child with OI. Over 95% said “yes” to being able to discuss these topics with the OI team. A small percentage reported “No”.
4. In the last 12 months has a member of the OI team talked to you about:
![This bar chart is showing parent and carer responses on whether they were informed by the OI team on transition from children’s to adult services and worries or concerns about their child moving from children’s to adult services. Around 40 to 50% said “yes” to being able to discuss these topics with the OI team. A smaller percentage, around 20 to 40% reported “No” and “can’t remember”.]](https://media.gosh.nhs.uk/images/GOSH_111125_4.4.Neurodisability.width-750.jpg)
This bar chart is showing parent and carer responses on whether they were informed by the OI team on transition from children’s to adult services and worries or concerns about their child moving from children’s to adult services. Around 40 to 50% said “yes” to being able to discuss these topics with the OI team. A smaller percentage, around 20 to 40% reported “No” and “can’t remember”.
Young people 12 years old and older (N=12):
5. In the last 12 months at school, has input from the OI team helped you in any of the following areas?
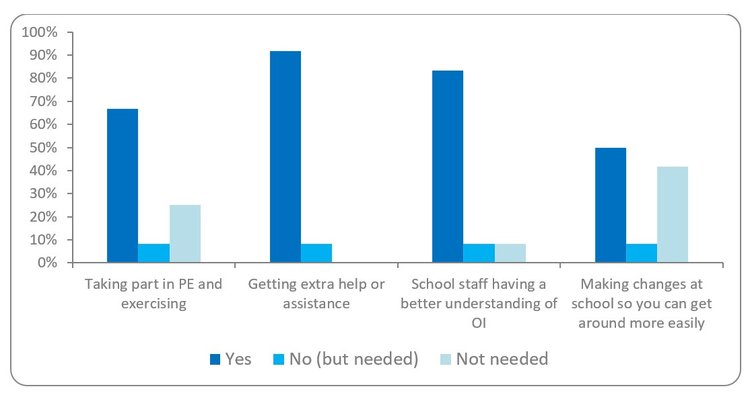
This bar chart is showing young people’s responses about school support needs. Around 60 to 80% said “yes” for support with PE and exercise, extra help, school staff having an understanding of OI, and making school changes for accessibility. A small percentage reported “no (but needed)”, and around 20 to 40% said support was “not needed”.
6. At your most recent visit to hospital or to clinic, did you have a discussion with a member of the OI team about:
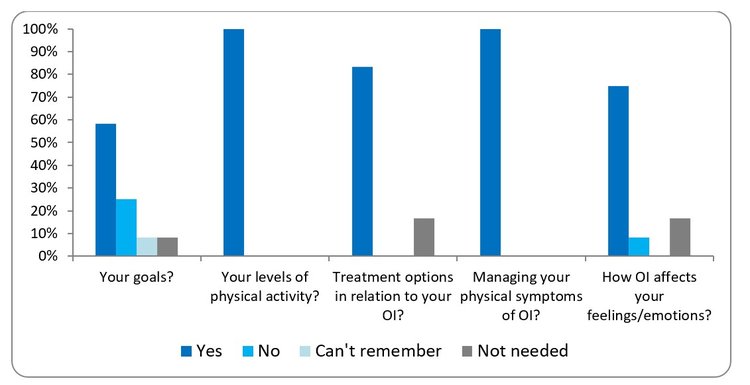
This bar chart is showing young people’s responses about their most recent visit at the hospital or clinic and whether they were able to discuss with the OI team about their OI, covering goals, physical activity levels, treatment options, managing symptoms, feelings or emotions and coping with feelings or emotions. Depending on the question, 60 to 100% answered “yes” to being able to discuss these topics with the OI team. A small percentage reported “no” or “can't remember” or “not needed”.
As an OI team we incorporate tools to aid personalised goal setting and encourage children and young people to participate more actively in the MDT Clinic appointment. This includes use of CanChild’s F-Words Goal Sheet, which focuses on individual goals across six domains: Functioning, Family, Fitness, Fun, Friends and Future. This has received positive feedback from children and young people with OI and their families.
7. Communication and empowerment
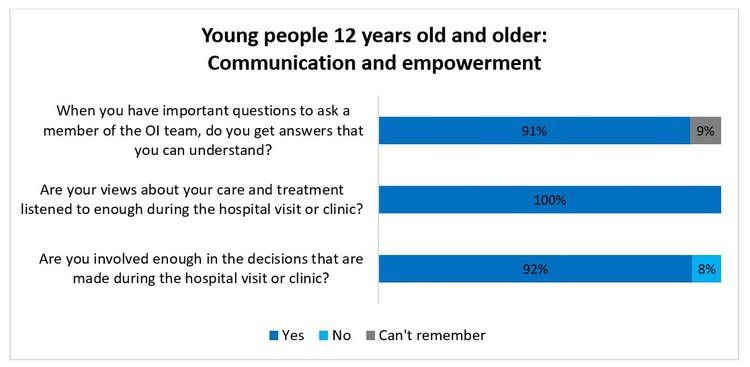
This bar chart is showing young people’s responses on communication and empowerment on whether they were able to have important questions answered by the OI team, views about their care and treatment being listened to, involvement in decision-making about their OI. Over 90% said “yes” to being able to discuss these topics with the OI team. A small percentage reported “No”, and, or “can’t remember”.
14-year-olds and older (N=8):
8. In the last 12 months has a member of the OI team talked to you about:

From the age of 12, the team begins to prepare young people and their carers for healthcare transition into adult services. To empower young people in the process, the Clinical Nurse Specialist (CNS) makes individualised time for young people, to support them in reflecting on their progress and health-related knowledge, emphasising self-advocacy and an increased sense of control to manage their own health.
At the final Paediatric OI Clinic appointment, young people are invited to complete an F-Words Goal Sheet and answer a Transition Key Question, which with their permission is shared with the OI Transition Team: “If you were meeting your OI Transition Team for the first time, what information about you would you like them to know?”
The OI Team has a well-established pathway for our young people to transition to adult services for ongoing care in adulthood. This includes a detailed handover to the adult team and a joint transition clinic. Paediatric allied health professionals meet with adult colleagues to hand over patients’ therapy needs in advance of clinic appointments. It is perhaps a learning point to note that not all patients are aware of the transition plan, though this may reflect a need for more young person-centred language as ‘transition’ may not be a phrase widely used or understood in this age group.
Continuous improvement
The Paediatric Osteogenesis Imperfecta National Team (POINT) has been developed as a national MDT of therapy, nursing, psychology, and social work professionals involved in the care of children and young people with OI. The current chair of POINT is the OI Clinical Specialist Physiotherapist at GOSH. The approach has been recognised by NHS England for its uniqueness and excellence in national collaborative MDT working for families with OI.
This information was published in November 2025.
Ref: 1125PAF0042
Last reviewed: Nov 2025