https://www.gosh.nhs.uk/conditions-and-treatments/clinical-outcomes/intensive-care-unit-clinical-outcomes/
Intensive Care Unit clinical outcomes
Clinical outcomes are measurable changes in health, function or quality of life that result from our care. Constant review of our clinical outcomes establishes standards against which to continuously improve all aspects of our practice.
About the Intensive Care Units
Clinical outcome measures
1. PIM3 Adjusted Mortality Rates for Paediatric Intensive Care
A key outcome measure used in Intensive Care Units (ICU) is the survival rate for patients, measured at the time when they are discharged. Raw mortality rates may be challenging to interpret as patients that are admitted in a sicker condition are at greater risk, and therefore the outcomes need to be ‘adjusted’ to consider the level of severity of the patients who are admitted to the intensive care unit.
The PIM3 (Paediatric Index of Mortality version 3) score is a nationally accepted risk score. This is calculated for every child admitted to ICU, to quantify the risk of death on admission. The PIM3 score is based on medical history, interventions and physiological measurements taken from time of first contact with an ICU doctor within the first hour after admission. The standardised mortality ratio (SMR) is the ratio of the number of actual deaths compared to the number of expected deaths based on the PIM3 score. The SMR helps us to evaluate if the survival rate is what would be expected according to how sick children are when they are admitted to intensive care.
The table and the funnel plots shown were provided by the Paediatric Intensive Care Audit Network body (PICANet) for admissions to the GOSH ICUs between January 2022 to December 2024.
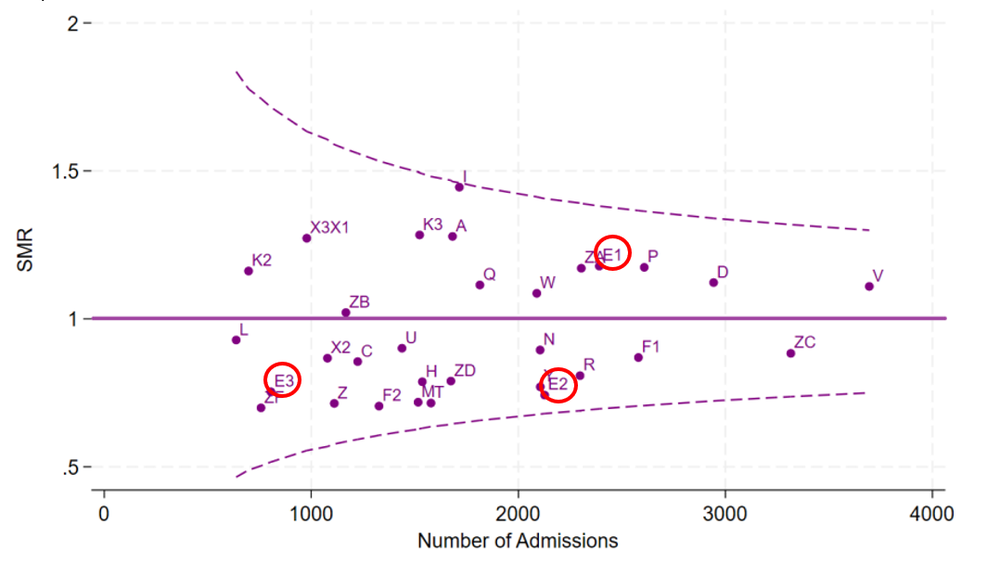
The funnel plot displays the SMR for each intensive care unit in the UK as a dot. If the actual number of deaths was the same as the predicted number of deaths, then the SMR would be 1, corresponding to the horizontal line in the middle of the funnel plot. The two dotted lines above and below the horizontal lines are called ‘99.9% control limits’. If an intensive care unit’s dot fell outside either of these lines, this would mean that the mortality rate would be very different to what is expected based on the case mix (upper line = much higher mortality than expected, and lower line = much lower mortality than expected). E1 is the GOSH Paediatric ICU (PICU), E2 is GOSH Cardiac ICU (CICU) and E3 is the GOSH Neonatal ICU (NICU). The dots for E1, E2 and E3 sit within the 99.9% control limits, so based on this threshold the SMR for all of these units is neither much higher nor much lower than expected.
Figure 1 Standardised Mortality Ratio (SMR) funnel plot for PICU (E1), CICU (E2) and NICU (E3) for Jan 2022 to Dec 2024, PIM3 Risk Adjusted (PIM3 Recalibrated 2025)
2. Emergency readmissions within 48 hours
Emergency readmissions to ICU within 48 hours of discharge is a quality outcome indicator that is monitored to help us evaluate how well the process of discharging children from intensive care is working. For example, if children were discharged from intensive care too early, then the percentage of readmissions would rise.
Table 1 shows the percentage of emergency readmissions to PICU within 48 hours of discharge. Table 2 shows the percentage of emergency readmissions within 48 hours for CICU. Table 3 shows the percentage of emergency readmissions within 48 hours for NICU. These data are displayed by year alongside the national average for that year across all paediatric ICUs in the UK and Republic of Ireland.
| Organisation | 2022 | 2023 | 2024 |
|---|---|---|---|
| National average (%) | 1.53 | 1.63 | 1.62 |
| PICU (E1) (%) | No data* | No data* | 2.4 |
*There is no data for PICU in 2022 and 2023 because these were a combination of PICU and NICU, which are reported separately from 2024.
The overall emergency re-admission rate is small. As with any rare event, variability can be high, which is reflected in our single centre data. The rate of emergency readmissions in 2023 and 2024 was higher than 2022. We seek to understand each case at our weekly mortality and morbidity meeting, where it is noted delayed discharges from PICU have also increased and are being investigated as causative, together with ongoing lack of a specifically commissioned HDU capacity.
| Organisation | 2022 | 2023 | 2024 |
|---|---|---|---|
| National average (%) | 1.53 | 1.63 | 1.62 |
| CICU (E2) (%) | 1.26 | 1.4 | 0.8 |
The percentage of children who were readmitted to CICU (E2) within 48 hours was similar to or lower than the national average in each of the three years.
| Organisation | 2022 | 2023 | 2024 |
|---|---|---|---|
| National average (%) | 1.53 | 1.63 | 1.62 |
| NICU (E3) (%) | No data* | No data* | 1.59 |
*There is no data for NICU in 2022 and 2023 because separate reporting for NICUs began in 2024.
The percentage of children who were readmitted to NICU (E3) within 48 hours was similar to the national average in 2024.
3. Unplanned extubation
Intubation is the placement of a flexible plastic tube through the mouth to maintain an open airway and provide ventilator-assisted breathing during critical illness. Extubation is the removal of that tube, which should happen in a planned way. Extubation can happen accidentally, which teams seek to avoid. The rate of unplanned extubations is therefore an important measure of care quality in the ICU environment. Unplanned extubation can happen when a child wakes up suddenly and all intensive care units expect to see this happen occasionally. However, if unplanned extubation is happening more often than expected this might mean that the care needs to be reviewed.
Table 4 shows the unplanned extubation rates (calculated per 1000 intubated days) for PICU (E1) alongside the average rate for all other intensive care units combined.
The rate of unplanned extubations in PICU (E1) for the reported year was lower than the national average.
| Organisation | 2022 | 2023 | 2024 |
|---|---|---|---|
| National average | 4.62 | 4.57 | 4.15 |
| PICU (E1) | No data* | No data* | 3.61 |
*There is no data for PICU in 2022 and 2023 because these were a combination of PICU and NICU, which are reported separately from 2024.
Table 5 shows the unplanned extubation rates (calculated per 1000 intubated days) for CICU (E2) alongside the average rate for all other intensive care units combined.
The rate of unplanned extubations in CICU (E2) for each of the reported three years shown was lower than the national average.
| Organisation | 2022 | 2023 | 2024 |
|---|---|---|---|
| National average | 4.62 | 4.57 | 4.15 |
| CICU (E2) | 1.7 | 3.3 | 2.32 |
Table 6 shows the unplanned extubation rates (calculated per 1000 intubated days) for NICU (E3) alongside the average rate for all other intensive care units combined.
The rate of unplanned extubations in NICU (E3) for 2024 was higher than the national average.
| Organisation | 2021 | 2022 | 2023 |
|---|---|---|---|
| National average | 4.62 | 4.57 | 4.15 |
| NICU (E3) | No data* | No data* | 10.37 |
*There is no data for NICU in 2022 and 2023 because separate reporting for NICUs began in 2024.
The unplanned extubation rate is higher than the national average on GOSH NICU. GOSH’s NICU is the only neonatal intensive care unit that contributes data to PICANet. So, the patient population may differ from the wider national PICU population. Studies from around the world have shown that there is a higher accidental extubation rate on NICUs compared to those seen on PICU. Nonetheless, we continue to undertake quality improvement work and education on our NICU to reduce this rate over time. Following improvements in tube fixation, sedation and in the techniques used to move babies for procedures and cares, internal data show that there has been a 50 per cent reduction in the accidental extubation rate on NICU from 2021 to 2024 and a further improvement has been seen in 2025.These extubation rates will continue to be closely monitored with an ongoing quality improvement project in place addressing this specific issue.
All data is published with the permission of PICANet from Paediatric Intensive Care Audit Network Annual Report 2025 (published December 2025): Universities of Leeds and Leicester.
The full report can be found here at Paediatric Intensive Care Audit Network (PICANet).
In 2016, a website called Understanding Children’s Heart Surgery Outcomes was launched to help parents and families to make sense of published survival data about children’s heart surgery in the UK and Ireland.
Continuous improvement
The ICUs are fully engaged in the Trust-wide quality improvement initiatives to improve the care of deteriorating patients on our inpatient wards. Together, these initiatives may reduce emergency readmissions to the ICUs.