https://www.gosh.nhs.uk/conditions-and-treatments/clinical-outcomes/gastrointestinal-allergy-nutrition-therapy-service-and-joint-allergy-group-clinical-outcomes/
GastroIntestinal Allergy Nutrition Therapy Service and Joint Allergy Group clinical outcomes
Clinical outcomes are measurable changes in health, function or quality of life that result from our care. Constant review of our clinical outcomes establishes standards against which to continuously improve all aspects of our practice.
About the GastroIntestinal Allergy Nutrition Therapy Service
The Gastro-Intestinal Allergy Nutrition Therapy Service (GIANTS) at Great Ormond Street Hospital (GOSH) is a specialist service that treats patients with Gastro-intestinal (GI) food allergy.
GI food allergy is an adverse reaction following the ingestion of a certain food, which presents with gastrointestinal symptoms such as diarrhoea, constipation, reflux, abdominal pain and vomiting. It often presents in early infancy. It is a complex, multifactorial, condition associated with reduced quality of life (QOL) and in some cases faltering growth. There is often significant clinical overlap of presenting symptoms with other gastrointestinal conditions; which can make diagnosis drawn out and confusing. The multidisciplinary team (MDT) at GOSH is comprised of: gastroenterologists, allergists, dietitians, psychologists and clinical nurse specialists. The service integrated these disciplines with the view to improve patient care, diagnosis and management of complex GI allergy conditions, with the aim of reducing the number of food exclusions, improving symptoms and subsequently improving QOL.
GI food allergy is an adverse immune response to a single, or sometimes multiple, food. Symptoms usually present within hours or up to three days following ingestion. The most common trigger foods include: milk, egg, wheat and soya. Diagnosis is made following a trial dietary exclusion of the suspected food/foods for a specified timeframe followed by careful challenge or reintroduction. This should be supported by specialist paediatric GI dietitians. Long-term exclusion of foods may be appropriate as a long-term treatment for a confirmed food allergy. However, long-term exclusion of foods is not without nutritional risk and should be limited where possible.
GIANTS food reintroduction clinical outcomes
To support the nutritional status of patients, the reintroduction of foods previously excluded should be considered with the support of the MDT. During April 2019 to April 2020, 76 patients cared for by GIANTS were supported in the reintroduction of foods into their diet.
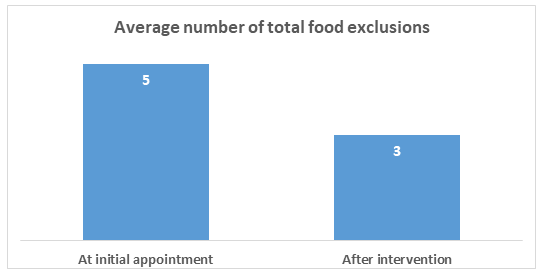
1. Average number of food exclusions
At initial appointment, the average number of foods excluded in the patients’ diet was 5 (range 1 – 17 foods, median 4). Over the 12 month study period, with support from the MDT and the specialist GI allergy dietitians, the average number of food exclusions reduced to 3 per patient (range 1 - 17, median 2.5).
Figure 1 Average number of food exclusions
2. Excluded foods
Milk/dairy was the most common excluded food in our cohort, with 78% (n=59) of the patients excluding this food group. The least common food excluded from the diet was fish/shellfish, with only 24% (n= 18) excluding this food group. 56% (n = 42) of patients excluded foods which were not within the top six common allergens (milk, egg, gluten, soya, nuts, fish/shellfish); excluded foods ranged from various fruits and vegetables to different types of animal meats.
Figure 2 Number of patients excluding each allergen

3. Food reintroduction
The GIANTS dietitians supported patients to reintroduce foods into their diets. Over the 12 month period, 55% (n=42) of patients managed to introduce at least one food into their diet. 16% (n=12) of patients reintroduced between 75 – 100% of excluded foods.
Figure 3 Number of patients reintroducing foods

The MDT approach has shown to be beneficial when supporting patients and their families to reintroduce foods into their diets following prolonged exclusion periods. The role of the MDT is to bring together professionals from different backgrounds to determine the most effective treatment plan for the patient. The introduction of foods improves overall nutrition and diet balance and evidence suggests that less food exclusions is associated with improved QoL for our patients and families.
4. Patient Reported Satisfaction
Between March 2019 and January 2020, patients attending GIANTS clinics were asked to complete a patient satisfaction survey. 91 patients were provided with the patient satisfaction questionnaire; 68% (n=61) of patients asked returned completed questionnaires. The results indicate that our communication and care was found to be very good. It also showed us that we can specifically make improvements in supporting our families and patients in feeling more prepared before clinic appointments. We will be using these results to consider how to improve our care.
Figure 4 Patient Satisfaction

References
Groetch, M. and Nowak-Wegrzyn, A., 2013. Practical approach to nutrition and dietary intervention in pediatric food allergy. Pediatric Allergy and Immunology, 24(3), pp.212-221.
Meyer, R. (2018). Nutritional disorders resulting from food allergy in children. Pediatric Allergy and Immunology, 29(7), pp.689-704.
M.G.Puoti, A Satar, L. Jackman, E. Saliakellis, O. Borrelli, L. Goh, D. Cutler. (2019). The burden of non-IgE mediated gastrointestinal food allergy on quality of life and psychological wellbeing in children. BSACI Annual Conference, Harrogate
Taberna, M., Gil Moncayo, F., Jané-Salas, E., Antonio, M., Arribas, L., Vilajosana, E., Peralvez Torres, E. and Mesía, R., 2020. The Multidisciplinary Team (MDT) Approach and Quality of Care. Frontiers in Oncology, 10.
This information was published in November 2021.