https://www.gosh.nhs.uk/conditions-and-treatments/procedures-and-treatments/halo-gravity-traction/
Halo gravity traction
This leaflet explains about the halo gravity traction system and aims to give you a better understanding of how it works. It’s not intended to replace the discussion between you and your healthcare team but may act as a starting point for discussion. If you have any questions or concerns, please speak with a member of your healthcare team.
What is halo gravity traction?
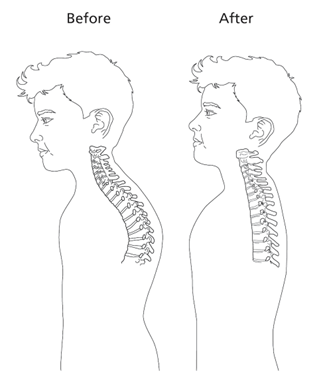
Halo gravity traction is a method of gently correcting the shape of a severely compressed or curved spine through stretching and straightening it. It is usually the first step in correcting a severe spinal deformity.
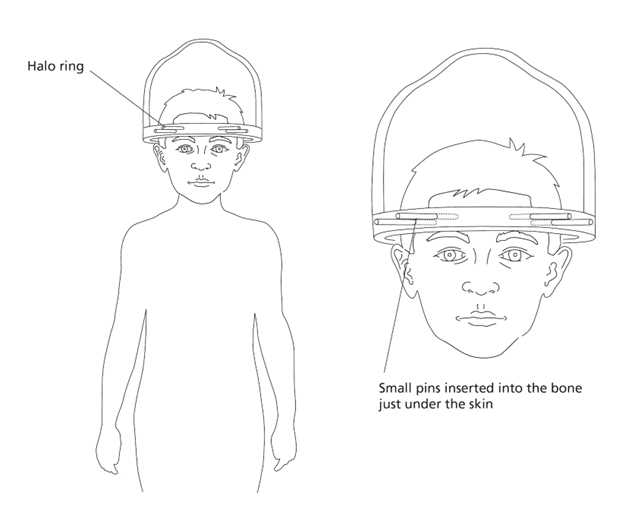
The halo gravity traction involves fitting a halo ring to the head under general anaesthetic – whilst your child is asleep. The halo ring is then attached to a pulley ‘traction’ system with weights, to slowly straighten the spine over several weeks.
The halo gravity traction is done whilst your child is an inpatient and they will need to stay in hospital the entire time, so doctors can monitor their progress and adjust the weight needed.
After halo gravity traction, children usually have a second surgical procedure called a ‘spinal fusion’. In this, the spine is fixed into its new position with metalwork, which permanently stabilises it.
Why do doctors use halo gravity traction?
In children who have very severe spinal curves – who the spinal surgeons think are suitable for halo traction – the halo gravity traction can be used to reduce the risk of damaging the spinal nerves and soft tissues during spinal surgery. It does not replace spinal surgery, but helps surgeons get better results and can make the surgery safer.
Spinal conditions that may require halo gravity traction include:
- Scoliosis
- Kyphosis
- Thoracic insufficiency syndrome associated with spinal deformity
- Congenital spinal deformities
- Neuromuscular scoliosis
Preparing for the procedure
Children are welcome to ask their doctors or nurses any questions they may have about halo gravity traction. We also refer all children who are undergoing halo gravity traction to a psychologist and play therapist. This is so that they can discuss the procedure, explore any concerns they may have and properly prepare. The psychologist, nurses and play specialist will also discuss with you how you can best support them during this time.
At the Spinal Investigation Day (SID), the nurses will take various measurements to ensure that the equipment fits your child correctly.
You will have received information in your child’s admission letter and at the SID about how to prepare for the operation. Please make sure to bring shirts and jumpers which button up the front, as putting clothes on over the head is difficult once the halo gravity traction is in place.
Eating and drinking before the procedure
Your child must not eat or drink anything for a few hours before the operation. This is called ‘fasting’ or ‘nil by mouth’.
Fasting reduces the risk of stomach contents entering the lungs during and after the procedure. You will be informed the night before the procedure of the time that your child should be ‘nil by mouth’.
It is equally important to keep giving your child food and drink until those times to ensure they remain well-hydrated and get adequate nutrition. This may involve waking your child in the night to give them a drink.
On the day of the procedure
The doctors will explain the operation in more detail, discuss any worries you may have and ask you to give your permission for the operation by signing a consent form.
Another doctor will visit you to explain about the anaesthetic. If your child has any medical problems, particularly allergies, please let the doctors know. Please also bring in any medicines your child is currently taking.
Fitting the halo ring
Once your child is under general anaesthetic, the surgeon will attach a light-weight halo ring to their head using small pins. The number of pins depends on your child’s size and can range between four and eight pins. If four pins are used, then two pins are secured through the skin into the bone on the forehead and two pins are placed into the bone at the back of the head.
What happens after the halo ring has been fitted?
Your child will come back to the ward to recover. The halo ring can be a little frightening to wake up in, so your child may need your reassurance. The nurses and play specialist will be there to offer reassurance and guidance to you and your child. Your child will likely notice the halo ring most in the first 24 hours and will become more comfortable with it as time passes.
Your child will have been given some pain relief at the end of the operation, so should not be in pain when they wake up. The nurses will regularly make sure that your child has enough pain relief to keep them comfortable. After a few days, paracetamol or ibuprofen-based medications should be enough to deal with any pain or discomfort.
Attaching the halo ring to the traction system
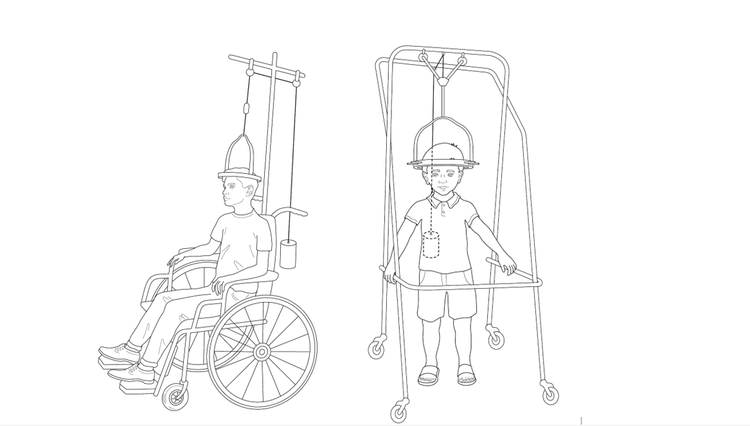
After the halo has been fitted, and when your child is ready and it is safe to do so, the spinal doctor will fix the halo ring to the pulley system. The pulley system can be placed on your child’s bed or onto a specially designed wheelchair.
Weights are then placed onto the pulley system to slowly straighten your child’s spine. The weight used will depend on your child’s body weight. The nurses and play specialist will be there to offer reassurance and guidance to you and your child throughout this process.
The spinal doctors will start off by applying a very low weight to the halo ring. Then each day they will increase the weight, until they reach the maximum target weight. The final weight is decided upon by your child’s consultant and depends on your child’s size, the spinal issue that is being treated and how they respond to the traction forces which are being applied to their spine. It can take one to two weeks to reach this final target weight.
The doctors will monitor your child’s movements and strength throughout the process and check how well they are tolerating the traction. They may take X-rays at different intervals to see how your child’s spine is responding. This will help them to decide how much more weight is needed and when your child is ready to have their second operation. In some cases, doctors may temporarily decrease the amount of weight to give your child’s body time to adjust.
The spinal doctors will also regularly check the halo pin-sites on your child’s head to make sure that they have not become loose. Every two weeks, they will ‘torque’ (tighten) the pins to make sure they don’t slip. This can be uncomfortable, so your child will be given pain relief before this is done. The discomfort usually only lasts for a few seconds whilst each of the pins is checked and tightened. In total, this tightening procedure should take less than five minutes. Your child may find this process quite frightening- the nurses and play specialist will be there to offer reassurance and guidance.
Once the spine has reached its best possible position, your child will have the spinal fusion surgery to permanently stabilise their spine.
Getting used to the halo gravity traction system
On the day after the operation, a Physiotherapist and Occupational therapist will visit your child. They will help your child to get used to the halo gravity traction system and get them ready to use the halo gravity traction in the wheelchair. There are special ways of moving about, getting up or sitting down while wearing halo system, and the physiotherapist will show your child how to do these things.
It may take you and your child some time to get used to halo gravity traction system. If you have any questions while your child is at the hospital, please speak to a member of the ward team.
For the halo gravity traction to work, it needs to be in place at least 23 hours a day.
Important
It is normal to feel pain and discomfort for the first few days after the halo ring is fitted, and pain medications will be prescribed to help with this. The pain and discomfort should get progressively better over time.
Let your child’s clinical team know immediately if:
- pain becomes extreme
- a pin feels loose, moves or looks inflamed
- you are concerned about the traction weights.
NEVER attempt to make any adjustments yourself.
NEVER help your child move by pulling on the halo ring.
Removing the halo gravity traction system
Your child will have X-rays to check that the spine is in the correct position, before it is removed.
Your child will then be given a general anaesthetic to have the equipment taken off. Sometimes, children do not feel that they need to have an anaesthetic when the halo equipment is removed, and it can be done when they are awake. This is only done if the child feels comfortable with this plan, and their family and clinical team agree that the child will be able to tolerate this procedure without an anaesthetic.
Frequently, the halo system is removed during the second operation to fix the spine in its new position, rather than during a separate procedure.
After the halo system is removed, the pin sites are massaged to help reduce scarring. No unusual care must be taken except what would be done for a small cut.
Your child’s neck may feel weak because the muscles haven’t been used as normal while the halo gravity traction system equipment was in place. The physiotherapist will see you before you go home to give you some advice and exercises. Occasionally, a neck collar is needed, but this is not usually required.
Your child will need to avoid high-impact activities for several months while their spine heals, and their muscles get stronger.
Patients are usually seen in the spinal clinic six weeks after they have been discharged home.
Are there any risks?
There are small risks associated with the procedure to attach the halo ring to the skull. The surgical team will discuss the risks with you at the Spinal Investigation Day (SID) before surgery and when your child is consented for surgery.
The major risks of the halo gravity traction procedure are:
- Infection in the skin, skull bone or very rarely the brain tissues.
- Bleeding in the skin, bone or extremely rarely in the brain.
- In the very rare event of bleeding or infection in the brain, this could lead to a stroke, which can be associated with a variety of symptoms including weakness and/or numbness (in the face, arms or legs), communication issues, vision issues and very rarely drowsiness.
- Pain at the pin sites – usually this resolves within a day of the halo ring being fitted.
- The halo pins becoming loose and moving.
- A scar on the skin from where the pins are sited.
- Pressure sores or skin breakdown.
- Neurological symptoms (usually these are temporary) – this can include weakness and numbness affecting the face, arms or legs, visual changes and very rarely bowel or bladder symptoms.
- Neck or back pain.
- Failure of it to improve the spinal shape.
- General anaesthetic risks (which the anaesthetist will discuss with you in more depth).
Bumps and knocks to the halo can be painful. Traumatic and boisterous activity should be avoided.
More information
Yes. The halo ring is not made from metal so your child can have a magnetic resonance imaging (MRI) scan while they are wearing it, if needed. The traction bail which attaches directly to the halo ring will need to be removed before the scan as it is not MRI compatible – this will be done by the spinal doctor if MR imaging is required and is not uncomfortable.
Your child will need to stay in hospital the entire time they’re in halo gravity traction, so doctors can monitor their progress and adjust the weight needed.
Halo gravity traction can be given when they are lying down in bed or when they are sitting in a specially designed wheelchair. Children are encouraged to be out of bed as much as possible. Most children find it easy to move around using the traction wheelchair once they adjust to being in traction.
Your child will have a special bed when they’re in traction. It can be difficult at first to get used to sleeping with the halo ring on. A rolled-up towel or small pillow can support your child’s head and make it easier for them to sleep.
Yes- children can shower or have sponge baths while in traction. It’s important to only use baby shampoo as other soaps may contain chemicals that could irritate the halo pin sites.
Hair washing can be tricky, but the nurses will show you how to do this. Your child’s hair can be washed gently, with care being taken not to bump or hit the pins as this may cause discomfort.
Once their hair has been washed, the pin sites should be checked by the nurses. No hair colouring, permanent dyes or treatments should be attempted while wearing a halo since this may lead to infected pin sites and discomfort around the pins. A hair dryer can be used on the ends of long hair, but the airflow must not be directed onto the halo equipment and is therefore not recommended for short hair.
At first, swallowing may feel different – your child might find it difficult to move their neck and it may take a little time for your child to adjust.
We don’t advise to routinely clean the pin sites, just gentle showering when hair washing. If the pin sites are oozing or painful or the pins are loose, let the nurse know.
Big, baggy clothes with buttons or zips are easier to wear over the traction equipment than tight fitting clothes. It may be best for your child to wear clothes a size or two bigger than normal.
Your child may be unsteady initially when upright and may take time to adapt to the halo system equipment. The Physiotherapist and Occupational Therapist will help them to adjust and give you advice for when you take your child off the ward in the traction wheelchair.
When your child wants to get into their chair, please let their nurse know. Do not attempt to transfer them from the bed to the chair without professional guidance and support.
Your child may find it difficult to read or work at a desk. Tilting the desktop may help and the Occupational Therapy team can provide advice.
The pins will leave small cuts in the skin when they are first removed. These typically scab over in a day or two. Your child will initially have small scars on their forehead, but these generally fade and become less noticeable over time.