https://www.gosh.nhs.uk/patients-and-families/your-care/clinical-outcomes/renal-dietetic-clinical-outcomes/
Renal dietetic clinical outcomes
Clinical outcomes are measurable changes in health, function or quality of life that result from our care. Constant review of our clinical outcomes establishes standards against which to continuously improve all aspects of our practice.
About the renal dietetic service
The Dietetic Department at Great Ormond Street Hospital for Children (GOSH) forms part of the Core Clinical Services Directorate. It is organised into clinical teams that each provide inpatient and outpatient services across many clinical specialties.
The Renal Unit at GOSH is the largest paediatric renal unit in the UK and one of the largest in Europe. Each year there are approximately 300-350 admissions to the renal ward; 100 admissions to outlying wards; over 7,000 outpatient attendances; and 70 patients on dialysis. The Renal Dietetic Service provides specialist paediatric renal dietetic support to children and young people and their families who are receiving treatment for kidney disease at GOSH.
Clinical outcome measures
The provision of safe, effective and quality care are key factors to excellent dietetic practice. Dietitians need to be able to identify and predict what the desired outcome of their intervention will be and then to what extent this is achieved. Measuring outcomes and sharing this information demonstrates the value of a dietetic service to the wider health community.
We aimed to assess whether dietetic input is effective in reducing raised blood potassium or phosphate in children with chronic kidney disease stages 3-5 and on dialysis (CKD3-5D). Reducing raised blood potassium and phosphate is important because high levels of potassium can be dangerous for the heart, including abnormal heart rhythms, and high levels of phosphate can affect the bones, growth and blood vessels.
Children and young people with CKD3-5D referred to a kidney dietitian at GOSH over a seven-month period (September 2023 – March 2024) for advice related to a high blood phosphate or a high blood potassium were included. Routine test results (including potassium and phosphate levels) were recorded at the initial review and again at follow-up. For haemodialysis patients, pre-haemodialysis bloods taken after a two-day break from dialysis were recorded. Dietetic goals, facilitators (such as improving kidney function, dialysis, medication, correction of acidosis, gastrointestinal symptoms) and barriers (such as worsening kidney function, dialysis, medication, acidosis, gastrointestinal symptoms, compliance, social issues) were documented.
Advice was given to 67 patients. Some patients were referred and reviewed (called episodes of care) multiple times within the data collection period. We had a total of 104 episodes of care included in this study. In 79 episodes of care, the aim was to reduce blood phosphate levels and in 25 episodes of care the aim was to reduce blood potassium levels. To be classified as having achieved the aim, the blood phosphate or potassium levels must have reduced below initial assessment levels. This meant that further intervention may have been required to achieve improvement in levels.
1. Reduction in blood phosphate level
Chronic kidney disease mineral and bone disorder (CKD-MBD) involves blood and bone abnormalities, and calcium build up in the blood vessels, which can cause hardening. This can lead to bone pain and deformities, fractures, short stature and cardiovascular problems.
Prevention and treatment of CKD-MBD includes lowering blood phosphate by control of dietary phosphate intake and administration of phosphate binder medication. Patients referred to the kidney dietitians with a high blood phosphate were included in the data collection and analysis.
In 79 episodes of care, the aim was to reduce blood phosphate levels. Sixty-five percent (51/79) of patients were given advice on correct administration or timing of phosphate binders in relation to phosphate intake from food and/or supplementary feeds, 42% (33/79) were given advice to reduce intake of phosphate-containing foods and 14% (11/79) had phosphate content of feeds reduced.
Eighty percent (63/79) of the patients achieved a reduction in blood phosphate levels following dietetic education (Figure 1). Of the 80% of patients who had a reduction in their phosphate levels, 68% (43/63) of these patients were on phosphate binding medication, 17% (11/63) of these patients had started or had adjustments to their dialysis during the study period and 3% (2/63) had an improvement in kidney function, which all may have facilitated the reduction in blood phosphate levels alongside dietary intervention.
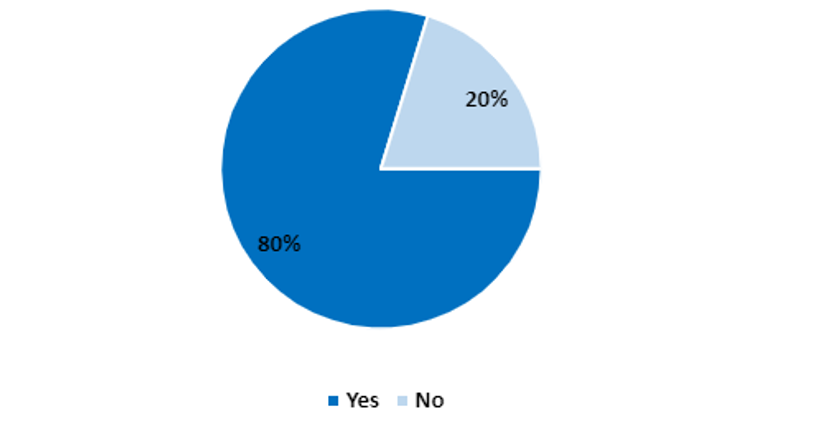
Fig 1. Percentage of patients that achieved a reduction in blood phosphate levels
Of the 20% (16/79) of patients who did not achieve a reduction in their blood phosphate levels, 50% (8/16) of these patients were non-compliant with dietary education or phosphate binding medication, 38% (6/16) had worsening kidney function and 6% (1/16) had changes to dialysis. These are all barriers to achieving reduction.
2. Reduction in blood potassium level
Potassium balance is disrupted in CKD and can result in hyperkalaemia (high potassium), which can cause life-threatening abnormal heart rhythms. Treatment of hyperkalaemia is guided by blood levels. Reduction in potassium intake alongside medical treatment is important to prevent hyperkalaemia.
Patients referred to the Renal Dietetics Team with a high blood potassium were included in the data collection and analysis.
In 25 episodes of care, the aim was to reduce blood potassium levels. Eighty-eight percent (22/25) of patients were given advice to reduce intake of potassium-containing foods and 20% (5/25) had the potassium content of their feeds reduced.
Ninety six percent (24/25) of the patients achieved a reduction in serum potassium levels following dietetic intervention (Figure 2). Of the 96% of patients who had a reduction in blood potassium levels, 17% (4/24) had started or had adjustments to their dialysis during the study period, 17% (4/24) had correction of their metabolic acidosis, 17% (4/24) had other medication changes, 13% (3/24) had improvement of gastrointestinal symptoms and 8% (2/24) had improving kidney function. These may have facilitated the reduction in blood potassium levels alongside dietary intervention.

Fig 2. Percentage of patients that achieved a reduction in serum potassium levels
Continuous improvement
We will collect outcome data for a three-month period each year to monitor results.
Due to staff shortages, not all patients referred to the Renal Dietetics Team with high blood phosphate or high blood potassium levels were included in the data collection, although they were seen and reviewed by the dietitian. At the next data collection period, we aim to include all patients referred and additionally report on:
- levels within normal range as well those with a reduction
- any changes to phosphate binder dosages
- specific compliance issues with phosphate binders
- details of potassium binders and any other changes in medication that can directly influence potassium
We will feed back our results to the national British Dietetic Association Paediatric Renal Nutrition Group (PRiNG) to encourage national engagement in benchmarking between centres.
We plan to develop a Patient Reported Outcome Measure (PROM) at the follow up dietetic review as part of the next annual update.
This information was published in May 2025.