https://www.gosh.nhs.uk/conditions-and-treatments/clinical-outcomes/tracheal-clinical-outcomes/
Tracheal clinical outcomes
Clinical outcomes are measurable changes in health, function or quality of life that result from our care. Constant review of our clinical outcomes establishes standards against which to continuously improve all aspects of our practice.
About the Tracheal Service
The Tracheal Team at GOSH was established in 2001 and is a group of health professionals brought together to provide the full range of expertise needed to treat conditions associated with the trachea (windpipe) and bronchi (branches of the windpipe to each lung).
The team sees and treats a wide variety of serious conditions, some very rare, including:
- long segment congenital tracheal stenosis
- tracheo-broncho malacia
- severe laryngo-tracheal clefts
- tracheal tumours
- cardiac problems causing bronchial and tracheal compression
- post FETO (fetal endoscopic tracheal obstruction –used to treat congenital diaphragmatic hernia in some centres) 'mega trachea'
The team comprises specialists in nursing, ear, nose and throat (ENT), interventional radiology, intensive care, cardiothoracic surgery, respiratory, anesthesiology, speech and language therapy, physiotherapy, general surgery, radiology and cardiology.
In 2006, the Tracheal Service received national recognition as the sole centre for the management of complex tracheal problems.
The chart below shows the year on year growth in referrals to the team.
Referrals to the Tracheal Team, Jan 1996 - December 2022

Clinical outcome measures
Long segment congenital tracheal stenosis (LSCTS) is the condition we see most often.
The team established the slide tracheoplasty surgical technique as the gold standard approach to treat LSCTS, and has the world’s largest experience of this type of surgery. The technique involves dividing the narrowed part of the trachea, which can sometimes be only 1 or 2 millimetres wide, and sliding the two sections over each other until the part of the trachea that is normal width is reached.
1. Early and late mortality for LSCTS
Table 1 below shows our results compared to other units around the world*.

We have the largest and longest series of children with congenital tracheal stenosis in the world. Our team has had the opportunity to build our expertise in the treatment of this condition. Internationally, we have produced some of the best outcomes for children with congenital tracheal stenosis and have been able to clinically follow-up children into adulthood (maximum follow-up of 282 months).
* We have defined early mortality as <30 days after operation, and late mortality >30 days. Other units may define early and late differently.
Reference:
Butler CR, Speggiorin S, Rijnberg FM, Roebuck DJ, Muthialu N, Hewitt RJ, Elliott MJ. Outcomes of slide tracheoplasty in 101 children: a 17-year single-center experience. The Journal of Thoracic and Cardiovascular Surgery 2014; 147(6): 1783-9.
2. Actuarial survival
Actuarial survival is a way of measuring survival that counts the proportion of patients alive (in relation to the expectation of life in a normal population) at a certain point in time, in this case after a slide tracheoplasty. Actuarial survival counts all deaths for a selected population, so this means that patients whose death was unrelated to their tracheal disease would also be counted in this figure.
For this graph, patients are counted as alive if they are in between follow up appointments, which are typically six-monthly clinic visits via the local hospital or at GOSH up to 18 years of age. Our patients are normally transitioned to adult healthcare at 18 years of age.
Between January 1995 and June 2019, we performed a total of 169 slide tracheoplasties with an overall survival of 89 per cent.
Fig 2.1 Overall actuarial survival

We are currently developing a risk score from our series to help inform pre-operative decision making. The figure below is an example of how this modelling can inform potential outcomes for a child referred to our unit. This modelling shows that children with the least number of risk factors have the best chance of a good outcome. Those children with cumulative risk factors have a higher chance of negative outcomes. The current model continues to evolve as we gain experience. The graph below shows the differences between those with and without risk factors, which are highly statistically significant (extremely unlikely to occur by chance alone).
Fig 2.2 Predictive modelling of risk-adjusted survival

3. Complications
One of the goals of an operation is to surgically correct the problem or improve function without causing problems associated with invasive procedures to the body. As our practice has evolved and our expertise has grown, we have seen a consistent reduction in surgical complications for slide tracheoplasty. During healing, it is expected that the trachea will narrow a little as part of normal scarring, and often the airway becomes a little soft or gets temporary obstruction with tissue called granulation tissue. These natural events are controlled by regular use of a small balloon in the airway for the first few weeks after surgery. A small minority of patients need a stent to keep the airway open. In the early days of our experience, we had to use metal stents that could not be removed once inserted. However, we have worked with a company in the Czech Republic (Ella CS) to make absorbable stents which are of great value in preventing the need for metal stents.
References:
Vondrys D, Elliott MJ, McLaren CA, Noctor C, Roebuck DJ. First experience with biodegradable airway stents in children. Annals of Thoracic Surgery 2011; 92(5):1870-4.
Rijnberg FM, Butler CR, Speggiorin S, Fierens A, Wallis C, Nouraei R, McLaren CA, Roebuck DJ, Hewitt R, Elliott MJ. The influence of stents on microbial colonization of the airway in children after slide tracheoplasty: A 14-year single-center experience. Pediatric Pulmonology 2015; Jan;50(1):79-84.
The figure below shows since 1995 the increasing number of slide tracheoplasties performed while the proportion of patients experiencing any complication consistently reducing.
Figure 3 Cumulative slides and cumulative complications, Jan 1995 - June 2019

3.1 Post-operative deep wound infection rate
Infection is a risk with any operation. The number and rate of patients who have a 'deep wound' infection is reported here. A deep wound is one that involves the deep soft tissues (fascial and muscle layers).
Table 3.1 Post-operative deep wound infection rate, January 1995 - June 2019
| Years | Number of patients | Number and percentage of deep wound infections |
|---|---|---|
| 1995-2007 | 43 | 7 (16.3%) |
| 2008-2012 | 51 | 2 (3.9%) |
| 2013-2017 | 60 | 4 (6.7%) |
| 2018-2019 | 15 | 1 (6.7%) |
| Total | 169 | 14 (8.3%) |
3.2 Re-admission to Cardiac Intensive Care Unit (CICU)
A small number of patients may be readmitted to CICU due to complications. The number and rate of these occurring within 30 days of surgery is reported here.
Table 3.2 Rate of re-admission to CICU within 30 days, January 1995 - June 2019
| Years | Number of patients | Readmissons to CICU within 30 days |
|---|---|---|
| 1995-2007 | 43 | 6 (14.0%) |
| 2008-2012 | 51 | 2 (3.9%) |
| 2013-2017 | 60 | 4 (6.7%) |
| 2018-2019 | 15 | 0 (0.0%) |
| Total | 169 | 12 (7.1%) |
4. Length of stay
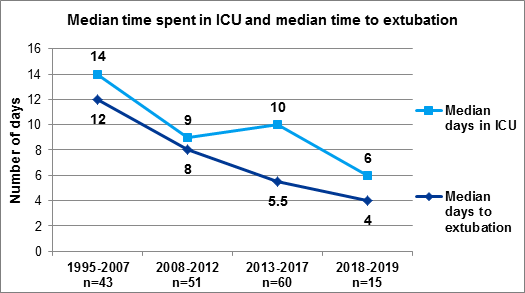
Another focus of the team’s commitment to delivering the best quality care has been to reduce the patients’ length of stay, with particular attention to the time spent on the intensive care units, and the time spent on a ventilator. The chart below shows our marked improvement over time in getting our patients well and fit for discharge after slide tracheoplasty. Extubation is the removal of the tracheal tube connecting a patient to a ventilator and means the patient is breathing spontaneously.
Figure 4 Time spent in ICU and time to extubation, Jan 1995 - June 2019
This information will be updated in June 2023.